
📋 Quick Summary
- Topic: How leukemia leads to anemia, the resulting symptoms, and how clinical teams manage leukemia-related anemia.
- Key Takeaway: Early recognition and medical consultation are critical for the best clinical outcomes.
- Remember: Always consult a qualified healthcare professional if you have concerns.
Leukemia and Anemia: Understanding the Connection
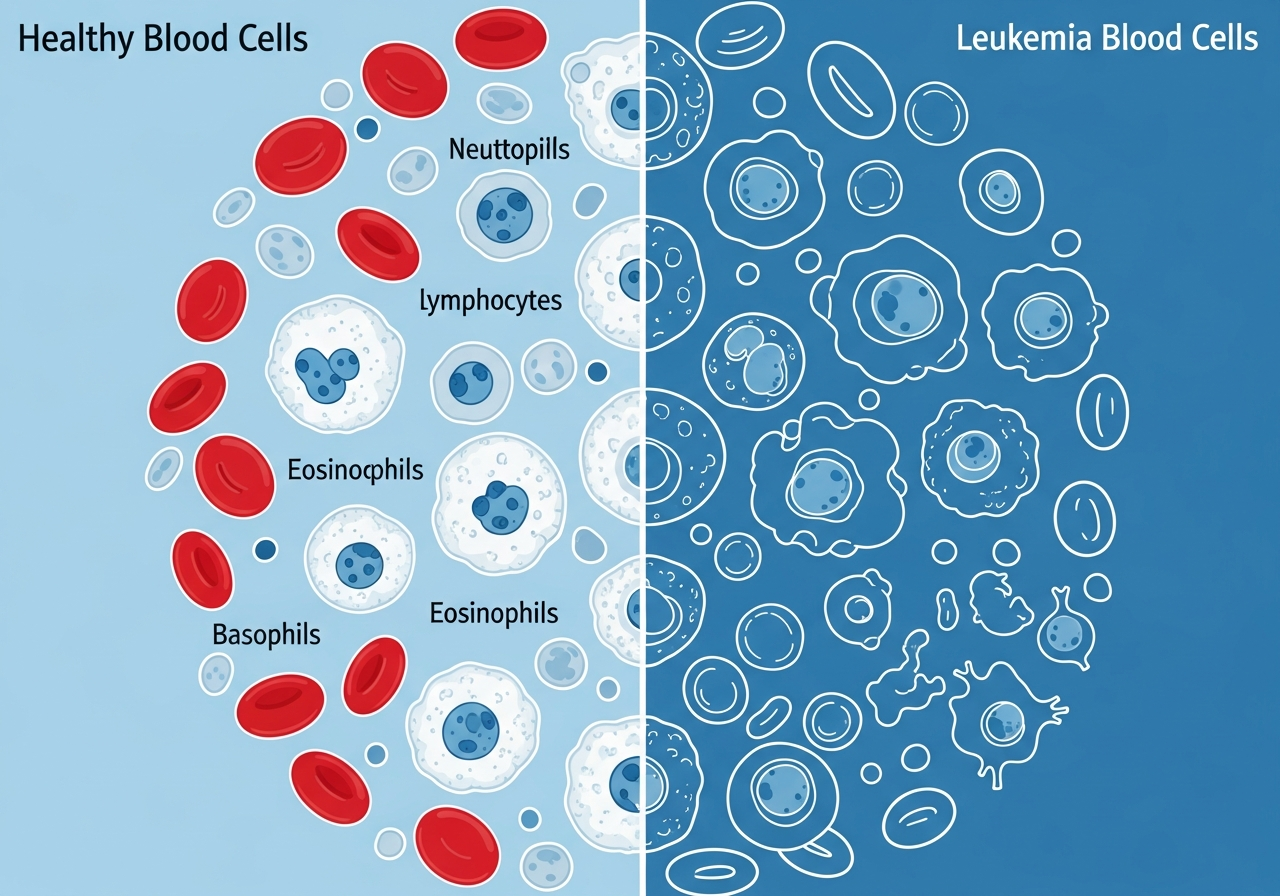
Anemia — a deficiency of functional red blood cells — is present in the vast majority of leukemia patients at the time of diagnosis and is one of the most clinically significant complications of the disease. It is the primary cause of profound fatigue, the driver of exertional breathlessness, and a contributor to the pallor and cardiovascular strain that characterize moderate to severe leukemia.
The connection between leukemia and anemia is direct and mechanical: leukemia cells proliferate in the bone marrow and crowd out the normal hematopoietic (blood-forming) stem cells that would otherwise produce red blood cells. Without these stem cells, the steady replenishment of the body's red blood cell supply — normally occurring at a rate of approximately 2 million new cells per second — falls far short of demand. The result is anemia that, left untreated, progresses from mild to severe and eventually to life-threatening cardiovascular decompensation.
Understanding anemia in the context of leukemia — how it develops, what it feels like, and how it is managed — empowers patients to recognize warning signs early and to engage actively with treatment decisions.
How Leukemia Causes Anemia: The Bone Marrow Mechanism
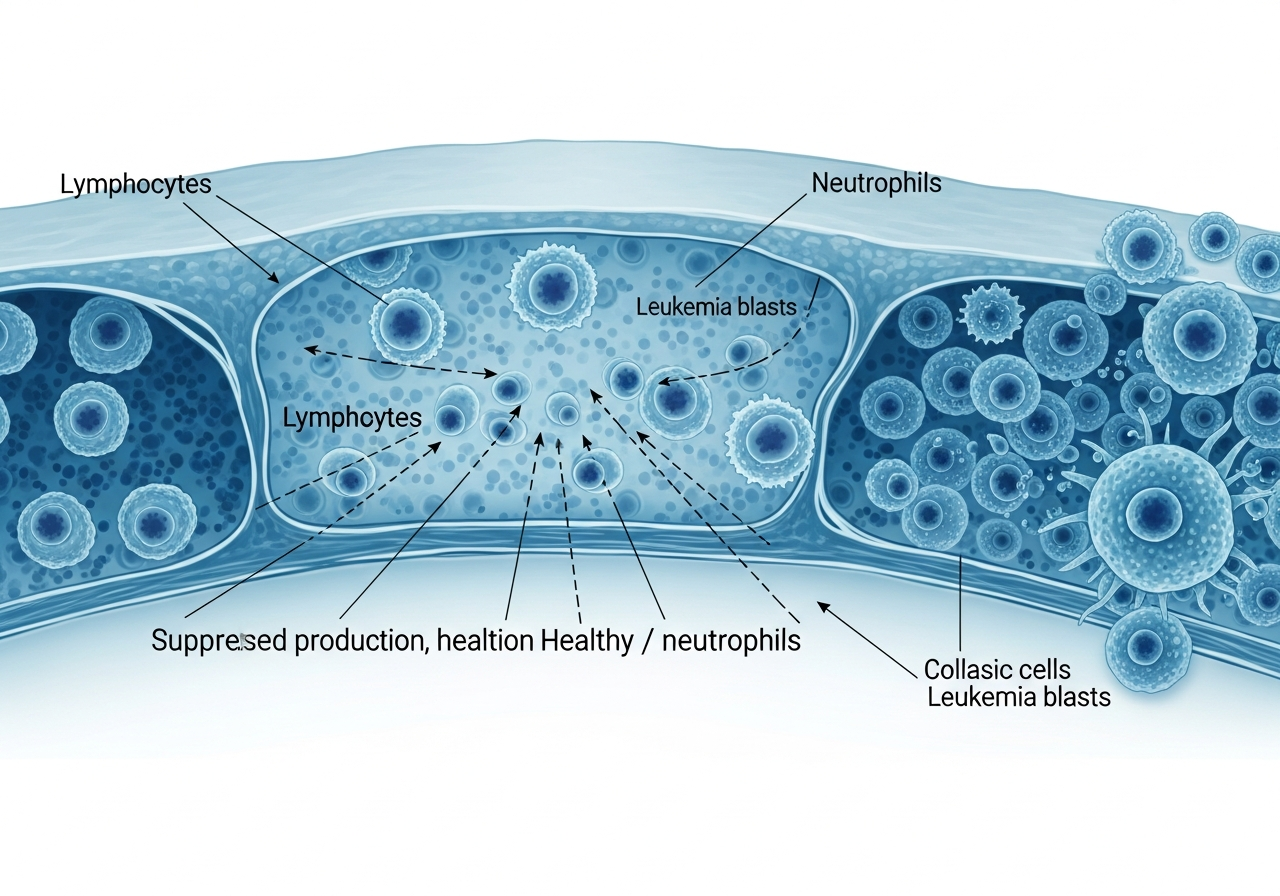
In a healthy individual, bone marrow contains a pool of pluripotent stem cells that continuously differentiate into all types of blood cells — red blood cells (erythrocytes), white blood cells (leukocytes), and platelets (thrombocytes). This process, called hematopoiesis, is exquisitely regulated to match production with demand.
In leukemia, one type of blood-forming cell undergoes malignant transformation and begins dividing uncontrollably. These leukemia cells — or "blasts" in acute leukemia — accumulate in vast numbers within the marrow space. As they proliferate, they physically displace and functionally suppress the normal stem cells responsible for erythropoiesis (red cell production).
The mechanism of suppression includes:
- Physical crowding: The marrow cavity has limited space. As leukemia cells expand, normal precursor cells are mechanically displaced.
- Cytokine-mediated suppression: Leukemia cells release inhibitory cytokines that suppress the differentiation and maturation of red blood cell precursors (erythroblasts).
- Competition for nutrients and growth factors: Leukemia cells compete for erythropoietin (EPO) signaling and growth factors that normal red cell precursors depend on.
- Immune-mediated hemolysis: In some leukemia types (particularly CLL), the immune system inappropriately attacks and destroys the body's own red blood cells — a condition called autoimmune hemolytic anemia (AIHA).
Symptoms of Leukemia-Associated Anemia
The severity of anemia symptoms correlates closely with the degree of hemoglobin deficiency and the speed of its development. Rapidly developing anemia (as in acute leukemia) produces more severe symptoms at any given hemoglobin level than slowly developing anemia (as in CLL) because the body has less time to compensate physiologically.
Common symptoms of leukemia-related anemia include:
- Fatigue and weakness: The most universal and often most disabling symptom — see our detailed guide on fatigue as a sign of leukemia.
- Pallor: Loss of normal skin color — most noticeable in the palms, nail beds, gums, and conjunctiva (inner eyelid). In individuals with darker skin tones, pallor is best assessed in the conjunctiva and mucous membranes.
- Dyspnea (breathlessness): Initially on exertion; in severe cases at rest. The body increases respiratory rate to compensate for reduced oxygen delivery per breath. Detailed in our guide on shortness of breath in leukemia.
- Tachycardia (rapid heart rate): The heart compensates for reduced oxygen per blood volume by pumping faster. Patients may notice palpitations or an awareness of their heartbeat.
- Dizziness and lightheadedness: Particularly on standing (orthostatic symptoms), from reduced blood volume and oxygen delivery to the brain.
- Cold extremities: The body redirects blood flow to vital organs (brain, heart) at the expense of peripheral circulation, leaving hands and feet cold even in warm environments.
- Cognitive impairment ("chemo brain" or anemia-related cognitive changes): Reduced oxygen delivery to the brain impairs concentration, memory, and processing speed.
- Chest pain or angina: In patients with pre-existing coronary artery disease, severe anemia can precipitate anginal symptoms by increasing cardiac oxygen demand relative to supply.
Types of Anemia in Leukemia
| Type | Mechanism | Associated Leukemia Type |
|---|---|---|
| Hypoproliferative (failure of production) | Bone marrow crowded by leukemia cells; reduced erythropoiesis | All types; most severe in AML and ALL |
| Autoimmune hemolytic (AIHA) | Immune system attacks and destroys own red blood cells (warm AIHA, cold agglutinin disease) | CLL; occasionally other types |
| Anemia of chronic inflammation | Cytokine-mediated reduced iron utilization; blunted EPO response | CLL, CML; any leukemia with systemic inflammation |
| Treatment-induced (chemotherapy-related) | Chemotherapy damages erythroid precursors; worsens existing bone marrow suppression | During chemotherapy for all types |
| Microangiopathic hemolytic (MAHA) | Mechanical destruction of red blood cells by fibrin strands in DIC | AML (particularly APL with DIC) |
Diagnosing Anemia in the Context of Leukemia
The complete blood count (CBC) is the primary diagnostic tool for assessing anemia. Key findings include:
- Hemoglobin (Hgb): The direct measure of oxygen-carrying protein. Normal values are approximately 12–16 g/dL for women and 13.5–17.5 g/dL for men. Leukemia patients may present with values of 6–10 g/dL or lower.
- Hematocrit (Hct): The percentage of blood volume occupied by red blood cells — closely mirrors hemoglobin trends.
- Mean Corpuscular Volume (MCV): The average size of red blood cells — may be normal, elevated, or reduced depending on the specific mechanism of anemia.
- Reticulocyte count: Counts the number of young red blood cells (reticulocytes). In hypoproliferative anemia, reticulocytes are inappropriately low for the degree of anemia — the marrow is not responding.
- Direct Coombs test: Detects antibodies on red blood cells. Positive in autoimmune hemolytic anemia — an important distinction for treatment planning.
- LDH and bilirubin: Elevated in hemolytic anemia from red blood cell destruction.
Understanding what these numbers mean and how they guide treatment decisions is explained in detail in our guide to understanding leukemia test results.
Treatment of Leukemia-Associated Anemia
Red Blood Cell Transfusions
The most immediate treatment for symptomatic severe anemia is a red blood cell transfusion. Most oncology teams transfuse when hemoglobin falls below 7–8 g/dL, or at higher thresholds if the patient is symptomatic (breathless at rest, chest pain, or severe fatigue). Each unit of packed red blood cells raises hemoglobin by approximately 1 g/dL. Transfusions provide rapid, reliable, temporary relief — but require ongoing re-treatment as long as the underlying leukemia suppresses marrow function.
Treating the Underlying Leukemia
The definitive treatment for leukemia-associated anemia is treating the leukemia itself. When chemotherapy, targeted therapy, or stem cell transplantation achieves remission, normal hematopoiesis resumes, and anemia resolves. This may take weeks to months as the bone marrow reconstitutes.
Autoimmune Hemolytic Anemia in CLL
When AIHA complicates CLL, treatment specifically targets the autoimmune response — typically with corticosteroids (prednisone), rituximab, or other immunosuppressive agents. In some cases, CLL-directed therapy (BTK inhibitors like ibrutinib) also improves AIHA.
Erythropoiesis-Stimulating Agents (ESAs)
In some settings — particularly in patients with myelodysplastic features or during low-intensity treatment — ESAs (epoetin alfa, darbepoetin) can stimulate red blood cell production and reduce transfusion requirements. However, their use is carefully considered in leukemia, as some data suggests potential for promoting proliferation in certain malignancies.
Anemia, Treatment Response, and Prognosis
The severity of anemia at diagnosis is one of several prognostic indicators in leukemia. More severe anemia often (but not always) reflects a higher leukemia cell burden. The speed of anemia recovery after treatment begins reflects how well the bone marrow is responding to therapy. Return of normal hemoglobin levels is one component of the definition of complete remission in acute leukemia.
Living with Anemia During Leukemia Treatment
Practical strategies for managing anemia's impact on daily life include:
- Pace activities to match energy levels — prioritize essential activities and take rest breaks
- Rising slowly from sitting or lying positions reduces dizziness from orthostatic hypotension
- Ensure adequate iron, B12, and folate from diet or supplementation — discuss with your oncology team
- Track hemoglobin trends between appointments to understand your trajectory
- Report any new or worsening breathlessness, chest pain, or palpitations promptly
Caregiver Guidance
Caregivers should be alert to signs that anemia is becoming severe: increasing pallor, shortness of breath with minimal activity, rapid resting heart rate, and fainting or near-fainting are signals that medical evaluation is urgently needed. Caregivers can assist by providing a home pulse oximeter (measures blood oxygen), monitoring breathing at rest, and facilitating quick access to emergency care when symptoms escalate.
When to Seek Urgent Medical Care
- Hemoglobin is known to be very low (below 7–8 g/dL) and the patient is symptomatic — breathless at rest, chest pain
- Sudden worsening of breathlessness at rest, severe pallor, or confusion in a patient with leukemia
- Palpitations, chest pain, or dizziness that is new or worsening
- Syncopal episode (fainting) in a known anemic patient
🚨 Emergency Warning Signs of Severe Anemia
- Breathlessness at rest or with speaking
- Chest pain alongside extreme pallor and fatigue
- Fainting or near-fainting
- Confusion or sudden extreme weakness
💬 Questions to Ask Your Healthcare Team
- What is my current hemoglobin level and what is the transfusion threshold for me?
- What is causing my anemia — marrow failure, hemolysis, or both?
- How often should my blood counts be checked while I am on treatment?
- Is my anemia expected to improve with my current leukemia treatment?
- Are there iron or vitamin supplements I should be taking?
- What level of activity is safe for me at my current hemoglobin?
This content is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or a qualified healthcare provider with any questions about a medical condition. Never disregard professional medical advice or delay seeking it because of information you have read on this website. Read our full disclaimer.
Frequently Asked Questions
Almost all leukemia patients experience some degree of anemia as bone marrow function deteriorates and red blood cell production declines.
Yes — fatigue, pale skin, and dizziness from anemia are often the earliest symptoms that prompt a blood test and leukemia diagnosis.
Immediate treatment may involve red blood cell transfusions; long-term management focuses on treating the underlying leukemia.