
📋 Quick Summary
- Topic: Understanding this slow-growing leukemia, the watch-and-wait approach, modern targeted treatments, and long-term prognosis.
- Key Takeaway: Early recognition and medical consultation are critical for the best clinical outcomes.
- Remember: Always consult a qualified healthcare professional if you have concerns.
Chronic Lymphocytic Leukemia (CLL): A Complete Guide
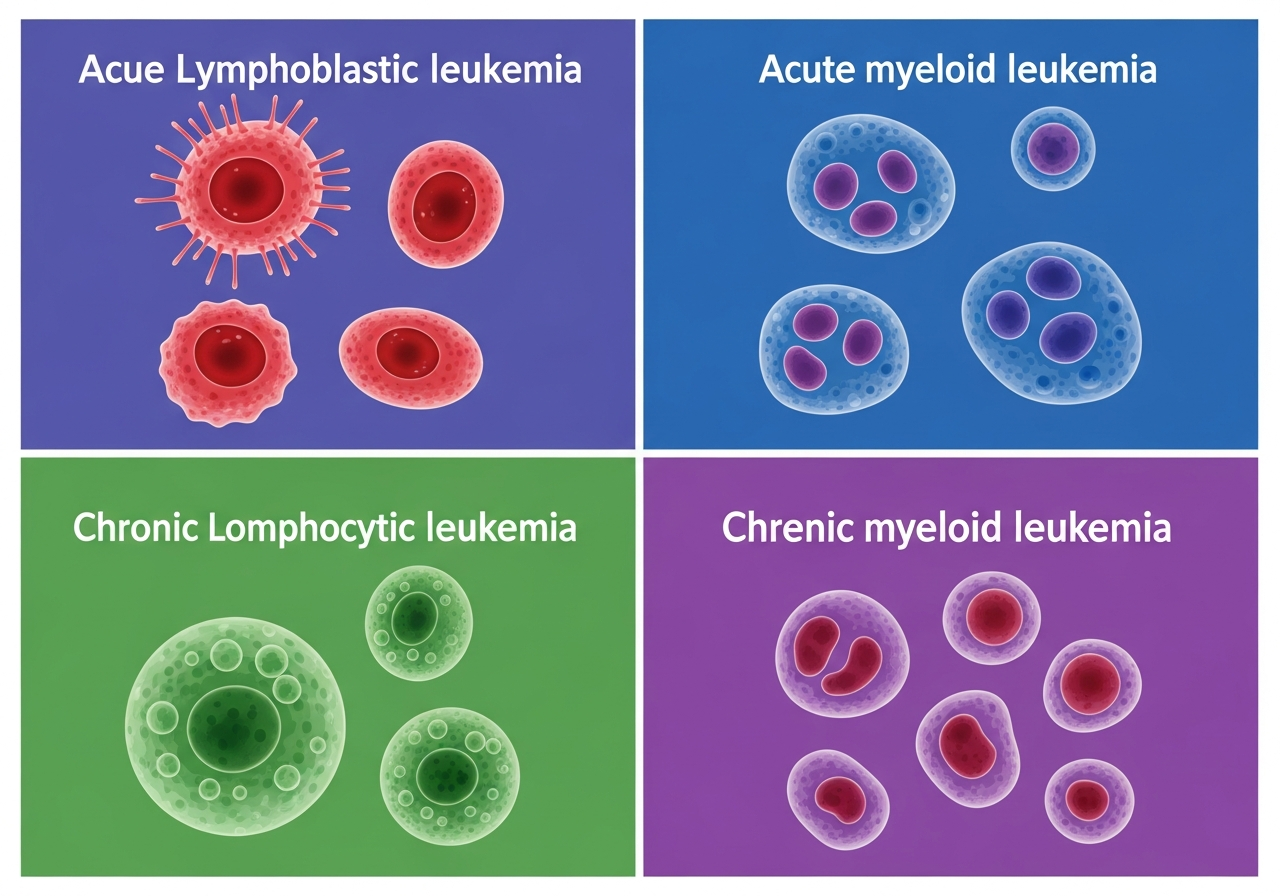
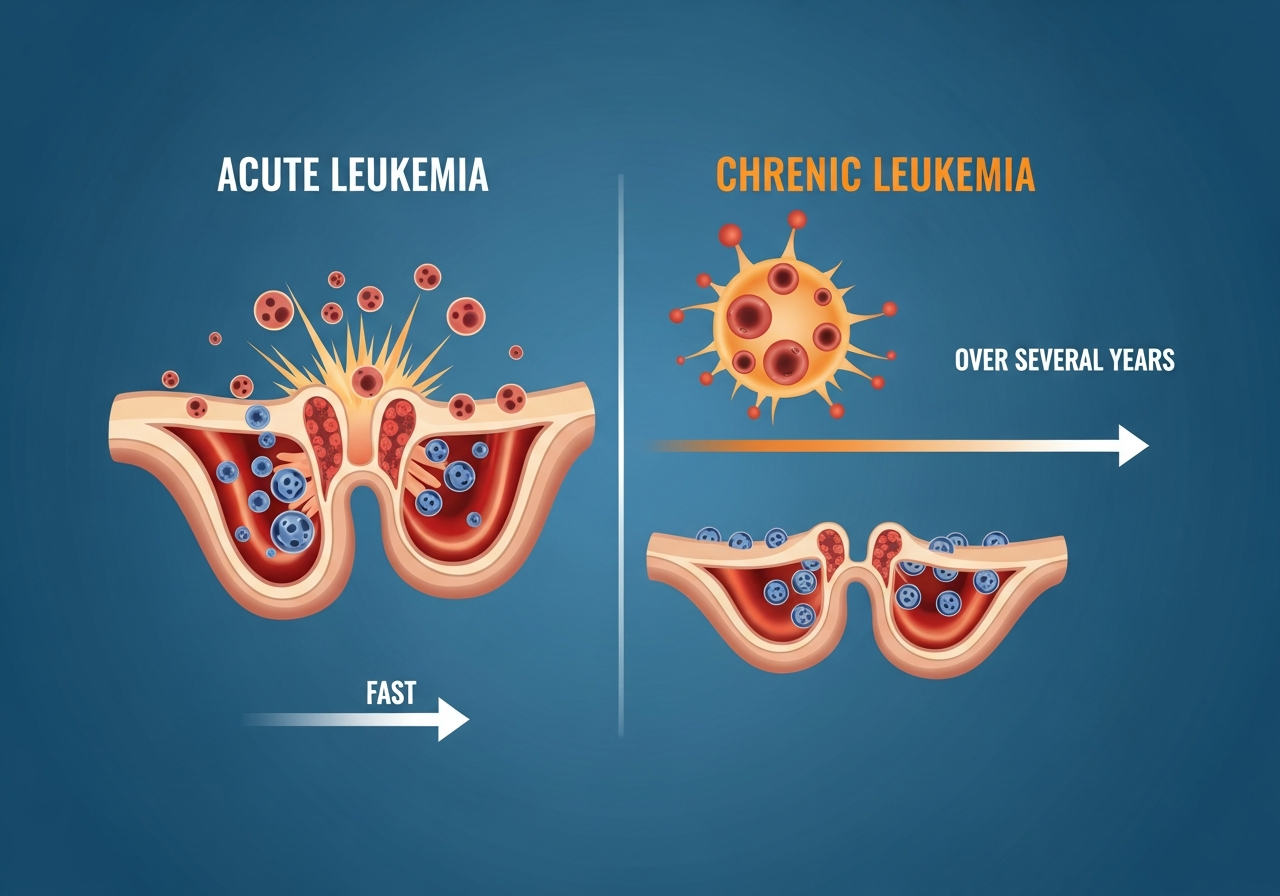
Chronic Lymphocytic Leukemia (CLL) is the most common leukemia in adults in Western countries. It is a cancer of mature but functionally abnormal B lymphocytes that accumulate progressively in the blood, bone marrow, lymph nodes, and spleen. Unlike acute leukemias, CLL typically progresses slowly — many patients live for years or decades after diagnosis with minimal impact on daily life. Some patients will never require treatment.
CLL is almost exclusively a disease of older adults, with a median age at diagnosis of approximately 72 years. It is diagnosed most commonly in people over 60, with fewer than 10% of cases occurring in people under 50. It is more common in men than women (roughly 2:1 ratio) and shows a striking geographic pattern — it is rare in East Asia but relatively common in North America and Europe.
The treatment landscape for CLL has been completely transformed in the past decade. The development of BTK inhibitors (ibrutinib, acalabrutinib, zanubrutinib) and BCL-2 inhibitors (venetoclax) has largely replaced conventional chemotherapy for most CLL patients, delivering higher response rates, more durable remissions, and better tolerability. Many patients with CLL can now look forward to decades of effective disease control with modern targeted therapy, even if cure remains elusive for most.
The Biology of CLL
CLL arises from the malignant transformation of a mature B lymphocyte — specifically, a memory B cell or B-cell progenitor that has undergone somatic hypermutation of its immunoglobulin heavy chain variable (IGHV) genes. The malignant B cells express characteristic surface markers: CD5 (normally a T-cell marker), CD19, CD23, and dim expression of CD20 and surface immunoglobulin.
Key biological drivers of CLL include:
- B-cell receptor (BCR) signaling: CLL cells are dependent on chronic active BCR signaling through a pathway that includes BTK (Bruton's tyrosine kinase). BTK inhibitors block this critical survival pathway, explaining their dramatic efficacy in CLL.
- BCL-2 overexpression: CLL cells strongly express BCL-2 — an anti-apoptotic protein that prevents cell death. Venetoclax directly inhibits BCL-2, forcing CLL cells into apoptosis.
- Microenvironment dependence: CLL cells depend on survival signals from the lymph node and bone marrow microenvironment — nurse-like cells, stromal cells, and T helper cells. BTK inhibitors partly work by displacing CLL cells from this protective niche, mobilizing them into the peripheral blood where they are more vulnerable.
Key prognostic markers in CLL biology:
- IGHV mutational status: Mutated IGHV (M-CLL) is associated with favorable prognosis; unmutated IGHV (U-CLL) indicates more aggressive disease.
- TP53 mutation / del(17p): The most important adverse prognostic marker — associated with resistance to chemoimmunotherapy and a requirement for targeted agent therapy. See genetics in leukemia for more on these mutations.
- del(11q): Associated with extensive lymphadenopathy and shorter remission with chemoimmunotherapy.
- del(13q) (isolated): Favorable prognosis; many patients remain stable for years.
- Trisomy 12: Intermediate prognosis; associated with some atypical CLL features.
CLL Staging: Rai and Binet Systems
CLL is staged using two systems — the Rai system (more commonly used in North America) and the Binet system (more common in Europe):
| Stage | Key Features | Risk Group |
|---|---|---|
| 0 | Lymphocytosis only (>5,000/μL monoclonal B cells) | Low |
| I | Lymphocytosis + enlarged lymph nodes | Intermediate |
| II | Lymphocytosis + enlarged spleen or liver | Intermediate |
| III | Lymphocytosis + anemia (Hgb <11 g/dL) | High |
| IV | Lymphocytosis + thrombocytopenia (platelets <100,000/μL) | High |
Symptoms of CLL
Many CLL patients — particularly those in Rai stage 0 or I — have no symptoms at diagnosis and are discovered incidentally on a routine blood test showing an elevated lymphocyte count. As the disease progresses, symptoms develop:
- Fatigue — the most common symptom; relates to anemia, immune dysfunction, and the systemic burden of disease
- Lymphadenopathy — painless, firm enlarged nodes in neck, armpits, and groin; a hallmark of CLL
- Splenomegaly and hepatomegaly — causing abdominal fullness and early satiety
- Frequent and severe infections — from hypogammaglobulinemia (lack of protective antibodies) and impaired T-cell function
- B symptoms: night sweats, fever, and unexplained weight loss — indicate more advanced disease
- Autoimmune complications: Autoimmune Hemolytic Anemia (AIHA) and Immune Thrombocytopenic Purpura (ITP) can occur and require specific immunosuppressive management
- Richter's transformation: In 3–10% of CLL patients, the disease transforms into an aggressive large B-cell lymphoma, presenting as rapidly worsening symptoms, dramatic lymph node enlargement, and constitutional symptoms — requires urgent evaluation
The Watch and Wait Approach
One of the most important and frequently misunderstood aspects of CLL management is active surveillance — "watch and wait." For patients in Rai stage 0–II without symptoms, multiple large randomized trials have shown that immediate treatment does not improve survival over deferring treatment until criteria are met. Beginning treatment for early-stage, asymptomatic CLL provides no benefit and exposes patients to treatment side effects unnecessarily.
Indications to initiate treatment (IWCLL criteria) include:
- Progressive marrow failure (worsening anemia or thrombocytopenia)
- Massive or progressive splenomegaly (spleen >6 cm below left costal margin)
- Massive lymphadenopathy (>10 cm) or rapidly progressive lymphadenopathy
- Lymphocyte doubling time <6 months (if starting from >30,000/μL)
- Autoimmune cytopenias poorly controlled by steroids
- Constitutional symptoms (weight loss >10%, drenching night sweats, fever without infection for ≥2 weeks)
During watch-and-wait, patients have regular monitoring visits (typically every 3–6 months) with blood counts, physical examination, and periodic imaging.
Diagnosing CLL
CLL diagnosis requires the presence of ≥5,000 monoclonal B lymphocytes/μL in the peripheral blood with a characteristic immunophenotype (CD5+, CD19+, CD23+, dim CD20, dim surface immunoglobulin). The diagnostic workup includes:
- CBC with differential: Elevated lymphocyte count, often predominantly small mature-appearing lymphocytes. Anemia and thrombocytopenia in advanced disease. Learn about CBC interpretation.
- Flow cytometry (peripheral blood): Definitive — confirms the CLL immunophenotype. A bone marrow biopsy is not strictly required for CLL diagnosis (unlike AML/ALL), as peripheral blood flow cytometry is sufficient.
- FISH and cytogenetics: del(17p), del(11q), del(13q), trisomy 12 — critical for risk stratification and treatment planning.
- IGHV mutational status: Mutated vs. unmutated — important prognostic information that guides discussion about treatment urgency and choice.
- TP53 mutation testing: By NGS — even without del(17p), TP53 mutation predicts poor response to chemoimmunotherapy and mandates BTK inhibitor or venetoclax-based treatment.
- CT scan: Assesses lymph node burden, spleen/liver size for staging and treatment decisions.
Treatment of CLL
BTK Inhibitors (First-Line Treatment Standard)
Ibrutinib (first-generation), acalabrutinib, and zanubrutinib (more selective, better-tolerated second-generation BTKi) have become the standard first-line treatment for most CLL patients requiring therapy. They are oral once- or twice-daily medications taken continuously until disease progression. Key features:
- Highly effective across all genetic subgroups, including del(17p)/TP53-mutated — making them particularly important for patients who cannot tolerate chemoimmunotherapy
- Expected transient lymphocytosis (lymphocytes move from nodes to blood) for first 1–6 months — this is not disease progression
- Bleeding risk and atrial fibrillation (ibrutinib) are important toxicities; acalabrutinib and zanubrutinib have improved cardiovascular safety profiles
- Indefinite continuous therapy — patients may remain on BTKi for many years
BCL-2 Inhibitor (Venetoclax)
Venetoclax + obinutuzumab (anti-CD20 antibody) is a time-limited (12-month) first-line regimen that achieves high rates of undetectable MRD. Venetoclax is highly effective and allows a finite treatment course (unlike continuous BTKi therapy), making it attractive for patients who prefer to avoid indefinite oral therapy.
The primary risk of venetoclax initiation is Tumor Lysis Syndrome (TLS) — rapid release of cell contents from dying cells that can cause acute kidney injury, cardiac arrhythmia, and seizures. Venetoclax is therefore started at a very low dose with gradual weekly escalation under careful medical monitoring.
Chemoimmunotherapy
Older regimens — FCR (fludarabine, cyclophosphamide, rituximab) and BR (bendamustine, rituximab) — are still used selectively in younger patients with mutated IGHV, where FCR can achieve very long remissions (possibly cure in some). However, they are ineffective in del(17p)/TP53-mutated disease and less durable overall than targeted agent approaches.
IVIG for Recurrent Infections
In CLL patients with significant hypogammaglobulinemia and recurrent serious infections, intravenous immunoglobulin (IVIG) infusions every 3–4 weeks supplement deficient antibody levels and reduce infection frequency.
Prognosis in CLL
CLL prognosis is highly variable. Median survival overall now exceeds 10 years, and with BTK inhibitor therapy, many patients achieve durable long-term disease control. Key prognostic factors:
- del(13q) isolated: Excellent; median survival >15 years with current therapy
- Mutated IGHV (M-CLL): More favorable biology; some patients never require treatment
- del(17p)/TP53 mutation: High-risk; requires BTKi or venetoclax; not curable with standard therapy; SCT may be considered
- del(11q): Intermediate; responds well to BTKi
- Richter's transformation: Poor prognosis; treated as aggressive lymphoma
Patient Considerations in CLL
CLL is a disease patients live with for many years — the psychological adjustment to a cancer diagnosis that may not require immediate treatment, and that may persist as a chronic condition for decades, is unique. Patients should be educated about watch-and-wait — that choosing not to treat immediately is evidence-based and protective, not neglectful. Annual influenza vaccination (inactivated) and pneumococcal vaccination are strongly recommended. Patients should avoid live vaccines. Proactive infection management — including prompt medical attention for any significant fever — is essential throughout the disease course.
Caregiver Guidance
CLL caregivers often face the unique challenge of supporting a loved one who is living with cancer but not yet treating it. This "watch and wait" period can be psychologically taxing — feeling like "doing nothing" when in fact monitoring is evidence-based and appropriate. Caregivers can help by attending medical appointments, tracking blood count trends over time, and monitoring for the symptoms (escalating lymphadenopathy, constitutional symptoms, worsening fatigue) that indicate the need for treatment initiation.
When to Seek Medical Attention in CLL
- Fever above 101°F in a CLL patient — immune compromise makes infections potentially life-threatening
- Rapid enlargement of lymph nodes over 2–4 weeks — possible Richter's transformation (emergency)
- Worsening fatigue or shortness of breath consistent with worsening anemia
- New bruising or bleeding beyond what has been previously discussed with the oncology team
- Constitutional symptoms beginning or worsening — may indicate need to start treatment
🚨 When CLL Patients Need Urgent Evaluation
- Fever above 101°F — immune compromise makes infection dangerous
- Rapid, dramatic lymph node enlargement — possible Richter's transformation
- Breathlessness or severe fatigue from worsening anemia
- Uncontrolled bleeding or rapidly increasing bruising
💬 Questions to Ask Your CLL Healthcare Team
- What is my IGHV mutational status and del(17p)/TP53 status, and what do they mean for my prognosis?
- Do I meet treatment criteria, or should I remain on watch and wait?
- If I need treatment, what is the best choice for my molecular profile?
- Should I receive IVIG given my low immunoglobulin levels?
- What vaccines should I receive, and which should I avoid?
- What changes in my condition should prompt me to call your office immediately?
This content is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or a qualified healthcare provider with any questions about a medical condition. Never disregard professional medical advice or delay seeking it because of information you have read on this website. Read our full disclaimer.
Frequently Asked Questions
No — many patients with early-stage CLL do not need immediate treatment and can be monitored for years under active surveillance.
A strategy of regular monitoring with blood tests and check-ups, reserving treatment until the disease progresses or causes symptoms.
CLL is generally manageable rather than curable. Many patients live for decades with good quality of life; BTK inhibitors have transformed outcomes.