
📋 Quick Summary
- Topic: Bruising, petechiae, pallor, and leukemia cutis — what these changes look like and when they signal blood cancer.
- Key Takeaway: Early recognition and medical consultation are critical for the best clinical outcomes.
- Remember: Always consult a qualified healthcare professional if you have concerns.
Leukemia and Skin Changes: A Clinical Guide
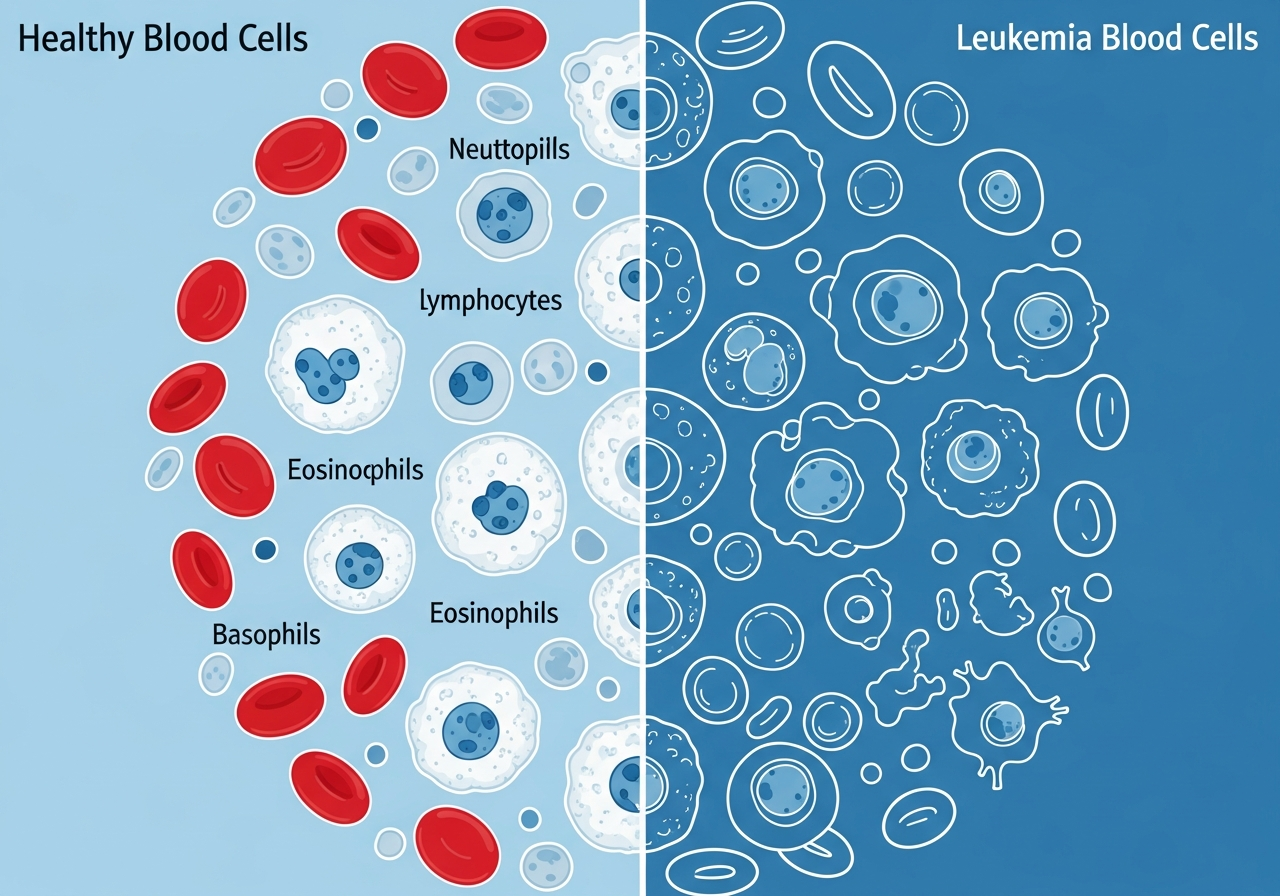
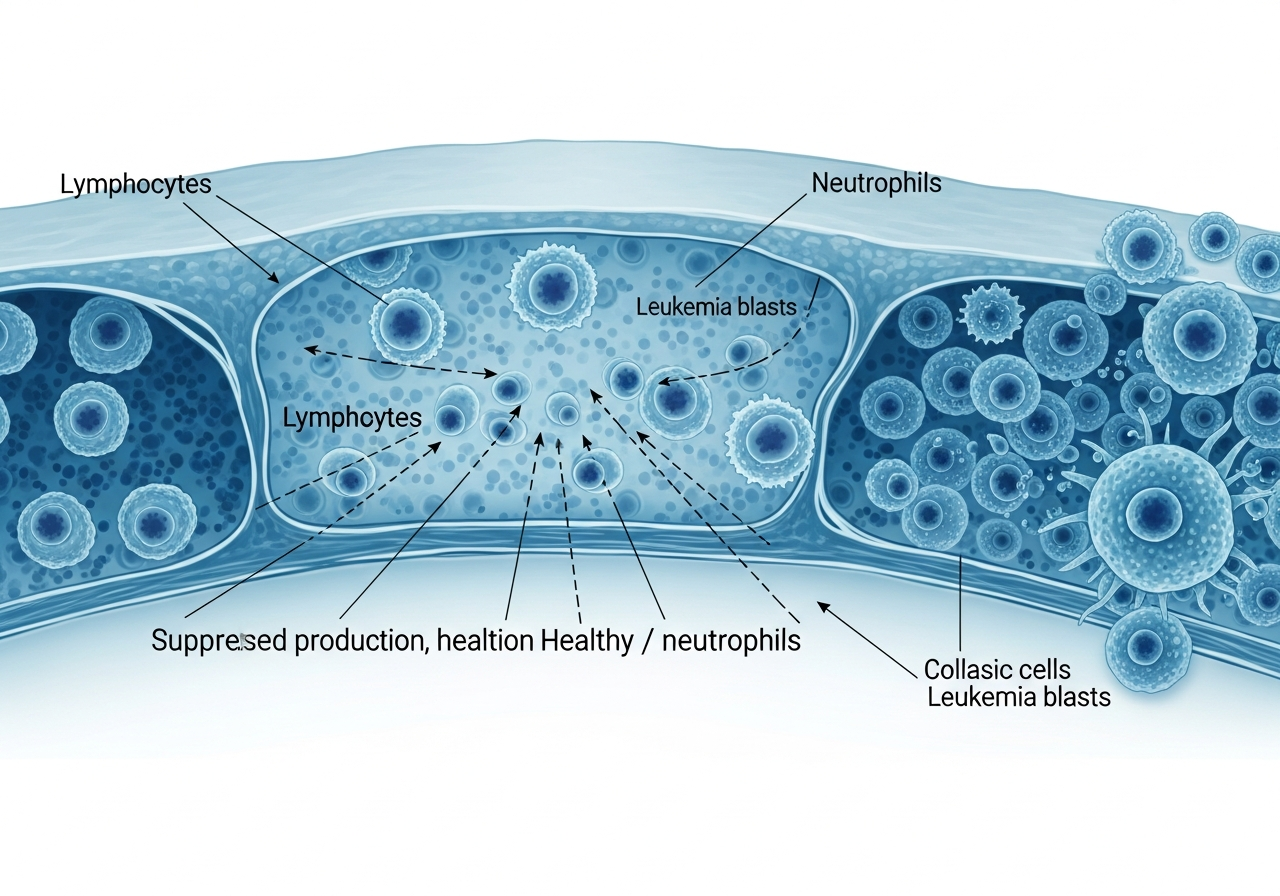
The skin is one of the most visible and diagnostically informative organs in leukemia. Skin changes — ranging from subtle pallor and petechiae to dramatic bruising and rare leukemic skin infiltrates — reflect the same underlying disruption that characterizes all leukemia: bone marrow failure producing abnormal blood cell populations and, in some types, direct infiltration of the skin by leukemia cells.
Recognizing leukemia-related skin changes is valuable for early detection. In many cases, visible skin findings — particularly petechiae and unusual bruising — prompt the initial medical visit and the blood test that reveals the underlying blood disorder. Skin changes can also signal disease progression, treatment complications, or the emergence of specific leukemia subtypes with cutaneous involvement.
This guide covers the full spectrum of skin changes associated with leukemia: from the common (bruising and pallor) to the rare but critically important (leukemia cutis) — and connects each to the broader context of early leukemia recognition, diagnostic evaluation, and treatment planning.
Petechiae and Purpura: The Diagnostic Red Dots
Petechiae are tiny, pinpoint-sized (1–3 mm) red or purple spots on the skin that do not blanch (turn white) when pressed. They result from microbleeds — small amounts of blood escaping from capillaries under the skin surface. Purpura are larger (greater than 3 mm) areas of similar discoloration. Both occur when platelet counts fall too low to seal these small capillary breaks — a direct consequence of the thrombocytopenia caused by bone marrow failure in leukemia.
Appearance and Location
Petechiae appear as flat (non-raised), pinpoint red or reddish-purple spots, most commonly on the lower legs, feet, and ankles (where hydrostatic pressure is highest), but they can appear anywhere on the body — including the palate (roof of the mouth) and conjunctiva (inner surface of the eyelids). They do not itch and are not palpable (cannot be felt by touch).
The "blanching test" is a simple way to distinguish petechiae from other red skin changes: press on the spot with a clear glass or your finger. If it blanches (turns pale), it is not petechiae — it reflects blood within vessels. If it does not blanch, the red color is from blood that has leaked out of vessels and is now under the skin — this is petechiae.
Clinical Significance
Petechiae in the context of other leukemia warning signs — such as fatigue, fever, or frequent infections — are a strong indicator for immediate blood count evaluation. When platelet counts fall below 50,000 cells/μL (normal is 150,000–400,000), petechiae typically appear. Below 10,000–20,000, the risk of spontaneous bleeding into organs is significant. Blood clotting problems in leukemia are among the most dangerous acute complications of the disease.
Abnormal and Unexplained Bruising
Easy bruising — technically termed ecchymosis — is one of the most common and earliest visible signs of leukemia. While bruising from trauma is normal, leukemia-related bruising has several distinctive features:
- Occurs without significant trauma: Large bruises appear from minimal contact — a light bump against furniture, carrying a bag, or simply the weight of blood pressure in dependent limbs.
- Disproportionate size: The bruise is far larger than the injury would typically cause.
- Unusual locations: Bruises appear on areas unlikely to sustain trauma — the torso, back, upper arms, or inner thighs.
- Slow fading: Normal bruises resolve in 1–2 weeks. Leukemia-related bruises persist much longer due to ongoing platelet insufficiency preventing resolution of the subdermal bleed.
- Concurrent petechiae: The simultaneous presence of large bruises and petechiae strongly suggests thrombocytopenia rather than simple trauma.
It is important to note that bruising can also worsen during treatment — chemotherapy further suppresses platelet production during the treatment nadir, often making bruising more prominent even as the leukemia itself is being controlled.
Pallor: The Visible Face of Anemia
Pallor — abnormal paleness of the skin — results directly from anemia, the reduction in red blood cells and hemoglobin that is nearly universal in leukemia. Hemoglobin gives blood its red color, and when hemoglobin levels fall significantly, the skin loses its normal pink tone.
Where to Assess Pallor
Pallor is most reliably assessed in areas where blood vessels are close to the skin surface:
- Conjunctiva (inner surface of the eyelid): Gently pull down the lower eyelid — the inner surface should be pink to red. Pale or white conjunctiva is a reliable sign of anemia across all skin tones.
- Nail beds: Normally pink; become pale or white in significant anemia.
- Palms of the hands: Palmar crease lines are normally reddish; pallor is noticeable when these lines are the same color as surrounding skin.
- Lips and gums: Loss of normal pink color is a reliable sign in all skin tones.
While pallor in fair-skinned individuals is obvious from the face, it can be missed in individuals with darker complexions if only facial skin tone is assessed. Conjunctival and palmar assessment is more reliable and should be performed regardless of baseline skin tone.
Leukemia Cutis: Direct Skin Infiltration
Leukemia cutis is a rare but diagnostically significant condition in which leukemia cells directly infiltrate the skin, forming visible and palpable skin lesions. It occurs in approximately 3–10% of patients with certain leukemia types and carries important prognostic and diagnostic implications.
Appearance
Leukemia cutis lesions vary in appearance but are typically:
- Firm, non-tender nodules or papules (raised bumps)
- Red, violet, brown, or grayish in color
- May appear as a diffuse infiltrated plaque or as scattered discrete nodules
- Most common on the trunk, extremities, and face
- In infants (congenital leukemia), skin involvement — called "blueberry muffin" lesions — is one of the most characteristic presentations
Clinical Significance
Leukemia cutis is most common in AML (particularly monocytic subtypes: FAB M4 and M5) and in congenital leukemia. In CLL, it can occur through direct skin infiltration by leukemic lymphocytes. The presence of leukemia cutis typically indicates a higher disease burden and may suggest systemic disease involvement. In some cases, skin lesions are the first presenting sign of leukemia — a "harbinger" diagnosis — before blood count abnormalities become apparent.
Leukemia cutis must be distinguished from non-specific skin changes of leukemia (bruising, petechiae, drug reactions) and from other skin infiltrates (sarcoidosis, granulomas). Skin biopsy with immunohistochemistry is required for definitive diagnosis.
Other Skin Changes in Leukemia and Its Treatment
Drug Reactions and Rashes
Many targeted therapies used in leukemia — including ibrutinib (BTK inhibitor), venetoclax (BCL-2 inhibitor), and imatinib (TKI) — can cause skin rashes ranging from mild erythema (redness) to more significant maculopapular eruptions. These are typically managed by the oncology team without discontinuing therapy unless severe.
Graft-versus-Host Disease (GVHD) Skin Manifestations
After allogeneic stem cell transplantation, the most common organ affected by GVHD is the skin. Acute GVHD typically presents as a maculopapular rash beginning on the palms, soles, and face that may spread to the entire body. Chronic GVHD skin manifestations can include scleroderma-like skin thickening, lichenoid changes, and altered pigmentation. GVHD skin changes require prompt evaluation and immunosuppressive treatment adjustment.
Herpes Zoster (Shingles) Reactivation
Leukemia patients — particularly those on T-cell depleting therapies or post-transplant — are at high risk for reactivation of latent varicella-zoster virus (VZV), producing herpes zoster (shingles). This presents as a painful, blistering rash following a dermatomal distribution (along a nerve path, usually unilateral). It requires urgent antiviral treatment and can be severe or disseminated in immunocompromised patients.
Chloroma (Myeloid Sarcoma)
Chloroma — also called myeloid sarcoma or granulocytic sarcoma — is a tumor-like mass of AML blast cells that can occur in the skin and soft tissue, presenting as a firm, greenish (from myeloperoxidase enzyme) or flesh-colored mass. It may occur before systemic leukemia becomes apparent or at relapse.
Diagnostic Evaluation of Skin Changes in Leukemia
The evaluation of skin changes in the context of possible leukemia includes:
- CBC with differential: Platelet count assessment for petechiae and bruising; hemoglobin for pallor; white cell count and differential for overall disease status. See our full guide on blood tests in leukemia diagnosis.
- Coagulation studies: PT, PTT, fibrinogen — if DIC is suspected (particularly in AML).
- Skin biopsy: Required for definitive diagnosis of leukemia cutis, chloroma, or to distinguish GVHD from infection post-transplant. Immunohistochemistry and flow cytometry on biopsy material characterize the infiltrating cells.
- Bone marrow biopsy: Central to confirming any new or changing leukemia diagnosis. Learn what to expect from bone marrow biopsy.
Treatment of Skin Changes
Treatment of leukemia-related skin changes focuses on treating the underlying leukemia and managing platelet levels. Platelet transfusions are given when counts fall below 10,000–20,000 cells/μL to prevent spontaneous bleeding into organs, or at higher thresholds if the patient is actively bleeding. Leukemia cutis and chloroma resolve with effective systemic leukemia therapy. GVHD skin involvement is treated with topical or systemic corticosteroids and other immunosuppressive agents under transplant team guidance.
Prognosis Context
Most leukemia-related skin changes — petechiae, bruising, pallor — are reversible with effective treatment and do not independently affect prognosis. Leukemia cutis and chloroma indicate higher disease burden and may be associated with a more aggressive disease course, but prognosis remains determined primarily by the underlying leukemia type and molecular features. The presence of skin changes at relapse (appearing after a period of remission) is an important clinical signal that requires urgent assessment.
Skin Care During Leukemia Treatment
Patients undergoing leukemia treatment should take precautions to protect fragile, easily bruised skin:
- Avoid activities with significant trauma risk during periods of thrombocytopenia
- Use electric razors instead of bladed ones; use soft toothbrushes
- Apply topical moisturizers to prevent dryness and cracking, which could become entry points for infection
- Inspect skin daily for new petechiae, bruising, rashes, or any new growths
- Wear protective gloves for kitchen and gardening activities
- Report any new rash, nodule, or unusual skin lesion promptly — some changes (GVHD, zoster) require urgent treatment
Caregiver Guidance
Caregivers should perform regular, gentle visual skin inspections — particularly of areas the patient cannot easily see themselves (back, scalp, feet). Document the date, location, and size of any new petechiae, bruises, or skin lesions. Photograph new lesions with timestamps, as this helps the medical team assess rate of change. Alert the medical team immediately to any rapidly spreading rash, painful blistering eruption (suggesting herpes zoster), or new nodular skin growth in a leukemia patient — these may require urgent medical intervention.
When to Seek Medical Attention
- New widespread petechiae or rapidly spreading purpura (emergency — possible severe thrombocytopenia or DIC)
- Bleeding from multiple skin sites or orifices that does not stop with pressure
- New painful, blistering, or ulcerating skin rash — possible herpes zoster requiring antiviral treatment
- New firm, nodular skin growth in a leukemia patient — possible leukemia cutis or chloroma
- Skin rash after allogeneic transplant — possible GVHD
🚨 Emergency Skin Signs in Leukemia
- Rapidly spreading petechiae or large purpuric patches — go to emergency room
- Uncontrolled bleeding from skin wounds
- Suspected DIC (widespread bruising, bleeding from multiple sites, possible in AML)
💬 Questions to Ask Your Healthcare Team
- What is my platelet count, and am I at risk for spontaneous skin bleeding?
- Should I have a skin biopsy to evaluate any unusual lesions I have noticed?
- Are any of my medications likely to cause skin reactions, and what should I watch for?
- What skin changes should prompt me to call immediately versus wait until my next appointment?
- If I have GVHD, what topical treatments are available for skin involvement?
- How will my skin changes improve as leukemia treatment takes effect?
This content is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or a qualified healthcare provider with any questions about a medical condition. Never disregard professional medical advice or delay seeking it because of information you have read on this website. Read our full disclaimer.
Frequently Asked Questions
They appear without trauma, are unusually large, occur in unexpected places, and take much longer than normal to fade.
A rare condition where leukemia cells infiltrate the skin, creating firm, red or purple bumps or patches on the surface.
Not necessarily — petechiae (tiny red dots from bleeding under the skin) and easy bruising can be early signs due to low platelets.