
📋 Quick Summary
- Topic: How genetic and molecular subtypes dictate treatment choice, the rise of personalized medicine, and classification systems.
- Key Takeaway: Early recognition and medical consultation are critical for the best clinical outcomes.
- Remember: Always consult a qualified healthcare professional if you have concerns.
Leukemia Subtypes and Treatment: Why Precision Matters
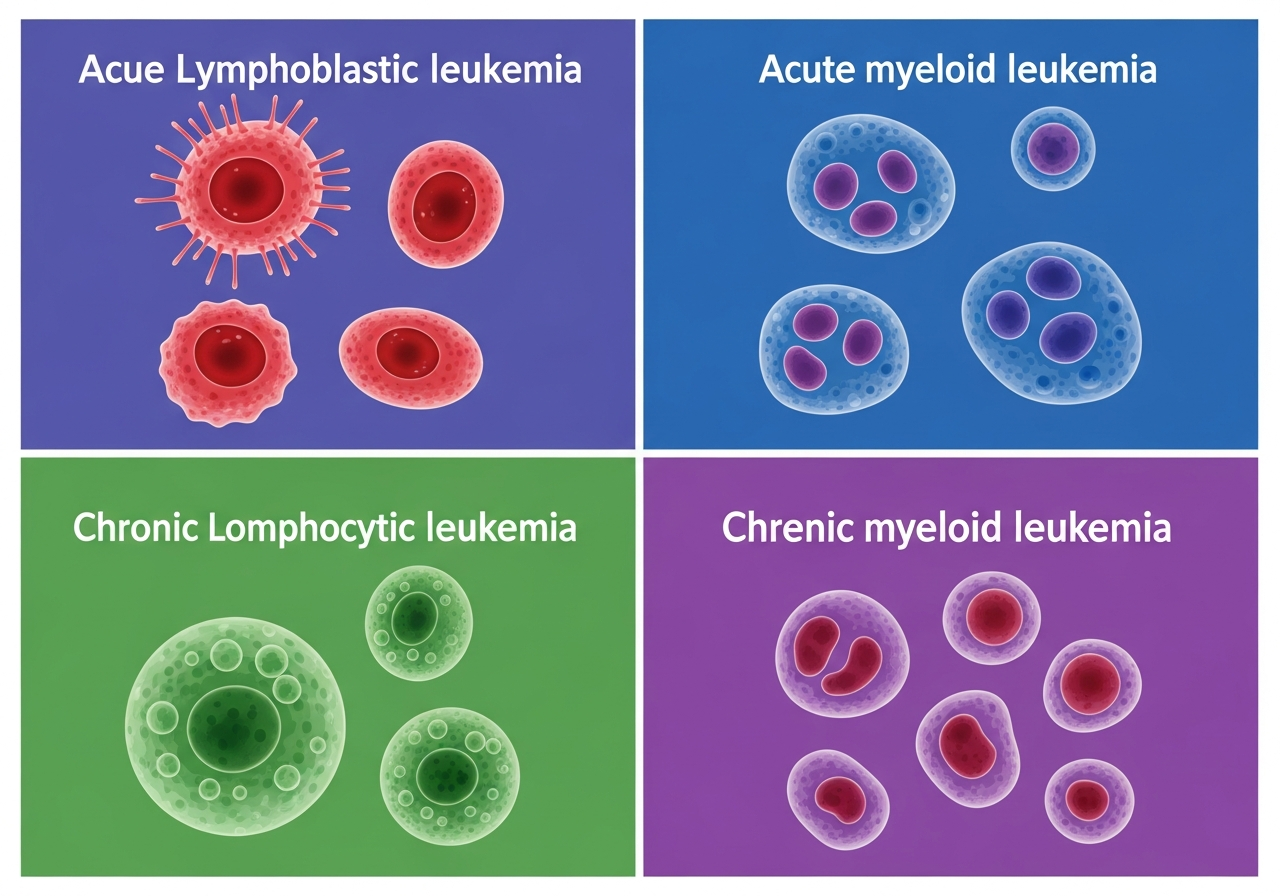
Among the most important advances in leukemia medicine over the past two decades is the recognition that "leukemia" is not one disease — it is hundreds of molecularly distinct diseases that share the feature of uncontrolled blood cell proliferation. Each leukemia subtype, defined by its specific pattern of gene mutations and chromosomal abnormalities, has a distinct response to chemotherapy, unique targetable vulnerabilities, characteristic prognosis, and optimal treatment strategy.
This recognition has driven the development of precision oncology in leukemia: the use of comprehensive molecular testing to identify the exact biological drivers of each patient's leukemia, followed by the selection of targeted drugs that attack those specific drivers. The result has been transformative — drugs that specifically target BCR-ABL1 in CML, FLT3 in AML, BCR signaling in CLL, and BCL-2 across multiple types have produced outcomes that conventional chemotherapy alone could not achieve.
Understanding leukemia subtype testing, risk stratification, and how subtype-specific treatments differ is essential for patients and families who want to engage meaningfully with treatment decisions and clinical trial discussions.
Why Leukemia Subtypes Matter for Treatment
The biological heterogeneity of leukemia has profound treatment implications. Two patients who both receive a diagnosis of "AML" may have diseases that are biologically as different from each other as two different cancer types. One may have a favorable molecular profile (NPM1 mutation, normal karyotype) that responds excellently to standard chemotherapy with cure rates exceeding 60–70%. The other may have a TP53-mutated, complex karyotype AML that responds poorly to the same treatment and has a 5-year survival below 15%.
Without subtype-specific information, both patients would receive the same treatment. With it, the first patient receives standard induction followed by high-dose cytarabine consolidation (avoiding the toxicity of transplant), while the second is enrolled in a clinical trial, receives a novel targeted agent, and is referred immediately for transplant planning.
The same principle applies across all leukemia types:
- In ALL: Philadelphia chromosome status determines whether TKI must be added; IGHV status predicts response to different agents; MRD levels guide intensification decisions
- In CLL: del(17p)/TP53 mutation determines that chemoimmunotherapy will fail and BTK inhibitor or venetoclax is required
- In CML: BCR-ABL1 mutation status (T315I vs. other resistance mutations) determines which TKI generation is needed
Molecular Testing: What Is Done and Why
At the time of leukemia diagnosis, a comprehensive molecular workup is performed on bone marrow and peripheral blood specimens. This workup includes multiple complementary testing modalities, each providing different information:
Conventional Cytogenetics (Karyotype)
Standard chromosome analysis examines all 46 chromosomes under a microscope for abnormalities in number (monosomies, trisomies) and structure (translocations, deletions, inversions). This broad survey identifies major chromosomal rearrangements — including the Philadelphia chromosome (t(9;22)) in CML and ALL, favorable inversions/translocations in AML, and complex/monosomal karyotypes associated with poor prognosis. However, conventional karyotype has limited sensitivity — it cannot detect small deletions or single-gene mutations.
Fluorescence In Situ Hybridization (FISH)
FISH uses fluorescently labeled DNA probes that bind to specific chromosomal sequences, allowing targeted detection of specific abnormalities with much higher sensitivity than karyotype. FISH panels are used to detect del(17p), del(11q), del(13q) in CLL; BCR-ABL1, MLL rearrangements, RUNX1-RUNX1T1, CBFB-MYH11, and PML-RARA in AML/ALL. FISH results complement karyotype for complete cytogenetic characterization.
Reverse Transcriptase PCR (RT-PCR)
RT-PCR detects specific gene fusion transcripts with extreme sensitivity — capable of detecting 1 leukemia cell among 100,000–1,000,000 normal cells. It is the standard method for quantifying BCR-ABL1 in CML (used for treatment monitoring), detecting PML-RARA in APL, and measuring MRD in specific ALL subtypes.
Next-Generation Sequencing (NGS) Panels
NGS simultaneously sequences dozens to hundreds of genes, identifying point mutations, small insertions/deletions, and copy number changes across the full cancer genome. NGS panels in leukemia typically cover 40–100+ genes including: FLT3 (ITD and TKD), NPM1, IDH1/IDH2, TP53, RUNX1, ASXL1, DNMT3A, TET2, SRSF2, U2AF1, SF3B1, CBL, KRAS, NRAS, BRAF, NOTCH1, FBXW7, and many others.
NGS results provide: (1) prognostic information (identifying favorable or adverse mutations), (2) therapeutic targets (FLT3 → midostaurin or gilteritinib; IDH1/2 → ivosidenib or enasidenib; TP53 → avoid intensive chemo, use novel agents), and (3) monitoring markers for MRD assessment.
Flow Cytometry (Immunophenotyping)
Multi-parameter flow cytometry identifies the surface protein "fingerprint" (immunophenotype) of leukemia cells, distinguishing B-cell from T-cell from myeloid origin and identifying specific surface targets for therapy (CD19 for blinatumomab/CAR-T; CD22 for inotuzumab; CD33 for GO; CD20 for rituximab/obinutuzumab). Flow cytometry is also the primary method for MRD assessment in ALL and CLL.
Risk Stratification: What It Means and How It Works
Risk stratification — classifying patients into risk groups based on their molecular, cytogenetic, and clinical features — is the central framework for treatment decision-making in leukemia. Each risk group is associated with a different expected outcome with standard treatment, and different risk groups receive different treatment intensity:
- Favorable (low) risk: Expected to respond well to standard therapy; cure is achievable without the most intensive approaches (e.g., without allogeneic SCT)
- Intermediate risk: Variable outcomes; treatment decisions are individualized based on response assessment and other factors; transplant may be beneficial
- Adverse (high) risk: Poor outcomes with standard therapy; requires the most aggressive available approaches, including upfront transplant planning and clinical trial enrollment
Precision Oncology in Leukemia: The Current Landscape
The precision oncology revolution has been particularly dramatic in leukemia, which — because of the accessibility of bone marrow samples and blood — has been at the forefront of molecular profiling. Key examples of subtype-specific targeted therapies:
| Leukemia / Mutation | Target | Drugs |
|---|---|---|
| CML / Ph+ ALL (BCR-ABL1) | BCR-ABL1 kinase | Imatinib, dasatinib, nilotinib, ponatinib, asciminib |
| AML (FLT3-ITD/TKD) | FLT3 kinase | Midostaurin (1L), gilteritinib (R/R) |
| AML (IDH2) | IDH2 enzyme | Enasidenib |
| AML (IDH1) | IDH1 enzyme | Ivosidenib |
| APL (PML-RARA) | PML-RARA / differentiation pathway | ATRA + arsenic trioxide |
| CLL (BTK-dependent BCR signaling) | Bruton's tyrosine kinase (BTK) | Ibrutinib, acalabrutinib, zanubrutinib |
| CLL/AML (BCL-2) | BCL-2 anti-apoptotic protein | Venetoclax |
| ALL (CD19) | CD19 surface antigen | Blinatumomab; CD19 CAR-T (Kymriah, Breyanzi) |
| ALL (CD22) | CD22 surface antigen | Inotuzumab ozogamicin |
| AML (CD33) | CD33 surface antigen | Gemtuzumab ozogamicin (GO) |
| HCL (BRAF V600E) | BRAF kinase | Vemurafenib, dabrafenib |
Minimal Residual Disease (MRD): Measuring the Depth of Response
MRD — the detection of residual leukemia cells below the threshold of standard morphological assessment — has emerged as one of the most powerful prognostic and therapeutic tools in leukemia management. MRD is measured by highly sensitive flow cytometry or PCR techniques capable of detecting 1 leukemia cell per 100,000–1,000,000 normal cells.
MRD negativity (undetectable residual disease) is strongly associated with long-term remission in ALL, AML, and CLL. In ALL, MRD assessment after induction guides intensification — MRD-positive patients receive more intensive consolidation; MRD-negative patients may receive less intensive treatment, reducing toxicity. In CLL, MRD negativity after venetoclax-based therapy is the primary endpoint that allows treatment discontinuation in fixed-duration regimens. In AML, MRD positivity in remission predicts relapse and may guide the timing of SCT.
How Subtype Determines Treatment Approach
The full spectrum of leukemia treatment options is discussed in our dedicated treatment guides. The key principle is that treatment selection begins with, and is always informed by, molecular subtyping:
- Chemotherapy agents are selected based on which combinations have been validated in clinical trials for the specific subtype
- Targeted therapies are selected based on the presence of the specific molecular target in the patient's leukemia
- Immunotherapy agents are selected based on surface antigen expression and subtype
- Stem cell transplantation is recommended based on risk category and treatment response
- Clinical trial enrollment is most urgently needed for high-risk subtypes without well-established standard therapies
Prognosis by Molecular Subtype
Prognosis is highly subtype-dependent and has improved dramatically as molecular understanding has evolved. The best outcomes are achieved when each patient's leukemia is precisely characterized and matched with the optimal treatment strategy for its specific biology. Patients with previously "incurable" subtypes — Ph+ ALL, FLT3-mutated AML, CLL with del(17p) — are now achieving much better outcomes with subtype-specific targeted therapies than with conventional chemotherapy alone.
The single most important action any leukemia patient can take — beyond receiving appropriate treatment — is ensuring comprehensive molecular testing is performed at diagnosis at a center with validated, updated molecular diagnostic capabilities. Without complete molecular profiling, optimal treatment selection is not possible.
Patient Considerations
Patients should feel empowered to ask specifically about their molecular test results and what each finding means for treatment selection. Questions such as "Was my FLT3 status tested?", "What is my ELN risk category?", and "Are there clinical trials for my specific subtype?" are appropriate and important. When results are complex, patients may request a patient-facing summary or ask their oncologist to explain each finding in plain language. Our guide to understanding test results provides a plain-language framework for interpreting common molecular findings.
Caregiver Guidance
Caregivers attending medical appointments can help by recording specific molecular findings and risk category in a dedicated health notebook. This information is needed at every specialist appointment and when seeking second opinions. Caregivers can also research the specific clinical trials available for their family member's subtype at ClinicalTrials.gov — armed with this information, they can have an informed conversation with the oncology team about whether any trials are appropriate. See clinical trials and treatment decisions for guidance.
When to Seek Urgent Medical Attention
Subtype information affects long-term management but rarely changes the urgency of acute symptom management. Regardless of subtype, any leukemia patient with fever above 101°F, uncontrolled bleeding, severe breathlessness, or sudden neurological change requires immediate emergency evaluation. See recognizing early leukemia symptoms for a comprehensive guide to warning signs.
🚨 Universal Leukemia Emergencies (Any Subtype)
- Fever above 101°F — febrile neutropenia is always an emergency
- Uncontrolled bleeding from any site
- Sudden severe headache or neurological change
- Severe breathlessness at rest
💬 Questions to Ask About Your Leukemia Subtype
- What specific molecular mutations were found in my leukemia?
- What is my risk category, and how was it determined?
- Is there a targeted therapy specifically approved or recommended for my mutation?
- How will you monitor my MRD, and what do my results mean for my treatment plan?
- Are there clinical trials specifically designed for my leukemia subtype?
- Should I seek a second opinion from a specialized leukemia center?
This content is for informational and educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your physician or a qualified healthcare provider with any questions about a medical condition. Never disregard professional medical advice or delay seeking it because of information you have read on this website. Read our full disclaimer.
Frequently Asked Questions
Specific genetic mutations determine which targeted therapies are most effective. Knowing the subtype allows precision treatment for the best outcome.
Analysis of leukemia cell DNA/RNA to identify actionable mutations (FLT3, IDH1/2, NPM1) that can be targeted with specific drugs.
Some molecular markers (like favorable cytogenetics in AML) predict excellent outcomes; others indicate need for aggressive early intervention.